


COVID-19 Vaccine mRNA Converts to DNA and Moderna Patented Genetic Sequence in SARS-CoV-2 and Vaccine mRNA - Part 2

In part 1, I reviewed the findings of a couple studies showing that SARS-CoV-2 RNA and the COVID-19 vaccine mRNA get reverse transcribed into DNA. One study confirmed the SARS-CoV-2 reverse transcribed DNA is expressed following reverse transcription, meaning it is either incorporated into cellular DNA or stays in the nucleus in such a way that it still gets expressed (i.e. extra-chromosomal DNA).

The other study did not confirm the reverse transcribed vaccine mRNA was incorporated into the host cell DNA or if it made its way into the nucleus as extra-chromosomal DNA. However, given the mRNA does get reverse transcribed, which originally, we were told was impossible, we now have a mechanism by which these products could alter our DNA.

Additionally, these findings also provide a possible explanation for why vaccine induced spike protein can be found in circulation for up to 4 months (i.e. mRNA gets reverse transcribed to DNA and the cells continue to express spike even though mRNA degrades quickly).
I also outlined some points to consider when theorizing what impact this could have.
The spike protein itself is a toxin (I addressed this in part 1).
Does the reverse transcribed mRNA code for anything other than spike, if so, is it possibly dangerous)?
Are all infected (by the vaccine) cells destroyed by the immune system or do some survive?
If they survive, where are they located in the body and, do they replicate?
When and how are the “new” DNA components expressed. Ex. always, sometimes, not at all? AND what proteins do they code for?
Could this impact germ-line cells (sperm/ova) making the DNA alterations heritable?
A Moderna Patented Genetic Sequence has been Found in SARS-CoV-2 and Maybe the COVID-19 mRNA Vaccines
To address the second point; What does the reverse transcribed mRNA code for (is any of it possibly dangerous)?
Igor does a great job of explaining that a Moderna patented genetic sequence has been identified in SARS-CoV-2 (spike protein).
He also provides a simplified’ish explanation of where exactly the SARS-CoV-2 sequence is found in the Moderna patent.

I strongly suggest reading his 3 articles on this topic before proceeding here.
I will briefly outline what is in these 2 articles.
The Sars-Cov-2 virus has a genetic insert (in the spike coding region) that exists ONLY in Moderna patent 9,587,003 from 2018. The specific genetic sequence is an MSH3 mutation and Moderna was using it to produce cancer related proteins and peptides for research on cancer vaccines (from what I understand).
Endogenously, in humans, MSH3 is one of the mutations known to cause Lynch Syndrome (LS). This is a genetic syndrome that increases the risk of multiple types of cancers over the course of a lifetime. It is characterized by mutations of four (MHS3 is one of them) mismatch repair (MMR) genes which code for proteins responsible for recognizing and repairing DNA lesions (Damage) occurring through multiple mechanisms including cell replication and oxidative stress (OS). Due to reduced MMR activity, LS patients have an increased risk of cancer because of a decreased ability to recognize and repair DNA lesions caused by multiple mechanisms.
The MSH3 mutation causing Lynch Syndrome is a loss of function mutation, meaning it decreases expression, while the MSH3 patent gene found in SARS-COV-2 is a gain of function mutation, meaning it increases expression. Both MSH3 mutations cause dysregulated expression of MSH3 which leads to reduced DNA repair capacity and increased cancer risk!!
Dr. Been explains this very well in the below video
This fits nicely with evidence that shows SARS-CoV-2 spike reduces DNA repair in infected cells.
More concerning, now that there is evidence that SARS-CoV-2 RNA may get reverse transcribed and possibly inserted into host cell DNA, will infected cells that escape initial death from the immune system continue to have a reduced ability to repair DNA; and therefore, an increased risk of becoming cancerous???
That last paragraph is all theoretical, I am not sure how much of the SARS-CoV-2 RNA gets reverse transcribed, how much could get incorporated into the host DNA, and whether the expression of that DNA would even produce spike or cause increased or decreased expression of MSH3? However, I can say this should be investigated ASAP!
Is The Moderna Patent in the Vaccines?
We also know that the spike mRNA in the Pfizer and Moderna vaccines closely match the genetic sequence of the SARS-CoV-2 spike protein which is where the Moderna sequence insert is found. So, the mRNA vaccines should also contain the MSH3 insert. I think… I would love to have someone confirm this for me!!!
Since, the vaccine mRNA has the potential to be reverse transcribed into DNA it may run the same risk as from the virus itself. Actually, a greater risk because the vaccine is guaranteed to be exposed to more body tissues because it gets into circulation, whereas the virus is most often confined to the respiratory system (depends on case severity. See my last post).
DNA Transcribed from Pfizer mRNA Vaccine Contains Mutant gp130 Tumor Gene
Remember my previous post commenting on the study showing that reverse transcription of Pfizer vaccine mRNA to DNA is possible. Well, the study also provided the DNA sequence that was reverse transcribed.
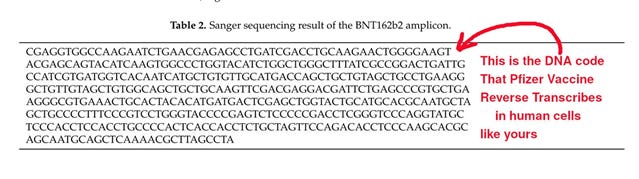
When investigating this sequence further, it was found that it contains a mutant version of the human gp130 gene. Igor does another great job of explaining how this gene was identified.
gp130 is involved in regulating inflammation and gene mutations altering its pathway are associated with multiple inflammatory and autoimmune conditions, including cancer. This is one of those situations, as with MSH3 and MMR discussed above, where too much is not good, and too little is not good, there must be balance.
So, given that the COVID-19 vaccine (Pfizer) mRNA may reverse transcribe into DNA that contains a possibly pathogenic gp130 gene mutation, we must ask what the consequences of this are. For now, we don’t know, but again this is something that needs to be investigated ASAP.
Let’s not go off the deep end here because we don’t know if the reverse transcribed DNA enters the nucleus in any useable form, whether it would even get transcribed into pathogenic proteins, or how long it would get transcribed for, if not incorporated into the host cell DNA (otherwise it would eventually be dissolved).
There are lots of unanswered questions here but, in my mind, they are very pressing, urgent questions that need to be answered asap!!
Unanswered Questions
Going back to the start of the article I listed a few points we need to consider when assessing what all this may mean. I touched on points 1 and 2 already.
Point 3: Are all infected (by the vaccine) cells destroyed by the immune system or do some survive?
We don’t know, some probably survive, but for how long? It likely differs from person-to-person as well.
Point 5: When and how are the “new” DNA components expressed? Always, sometimes, not at all? What proteins do they code for?
We don’t know for sure yet, most of my 2-part series speculated on this question.
Connecting COVID-19 Biodistribution to Reverse Transcription Concerns
Point 4: If they survive, where are they located in the body?
Point 6: Could this impact germ-line cells (sperm/ova) making the DNA alterations heritable?
The following is nothing new, it has been known since at least May 2021 that the mRNA vaccines do not simply stay in the injection site, they circulate around the body and accumulate in certain tissues.
Concerns about biodistribution first came to light when Canadian vaccinologist, Dr. Byram Bridle got his hands on a freedom of information request out of Japan that showed the biodistribution of the lipid nanoparticle (LNP) used in the mRNA vaccines. The document showed the LNP travelled to multiple body tissues including adrenal glands, liver, bone marrow, lymph nodes, ovaries, spleen, and thyroid. There were many other locations, these tissues simply had the highest concentrations 48 hours after injection.
There were criticisms about this information as the dosage used in the rodents was higher than what would be contained in Human injections (relatively speaking), and also it didn’t confirm if the mRNA also travelled to those tissues.
However, since then, multiple studies and freedom of information releases have shown that the LNP and the mRNA circulate to areas other than the injection site, and even continue to produce spike.

So, the answer to point 4 is:
The vaccine accumulates in many parts of the body and it is likely that certain vaccine “infected” cells survive for some amount of time and continue to produce spike.
The answer to point 6 is even more concerning since it appears that the vaccine can accumulate at least in the ovaries (maybe testes?).
What does this mean? It’s not certain. But, we know the spike protein is toxic and it can impair DNA repair, we also know the genes (discussed above) found in the vaccine and spike protein can negatively impact inflammation. Therefore, it is possible the vaccines may kill/damage ova (reducing the female lifetime fertility period), or possibly even contribute to damaged ova DNA which is something that can be passed to offspring.
Additionally, the reverse transcription study suggested that the mRNA vaccine might increase LINE-1 expression and we know LINE-1 is involved in embryonic development and we certainly don’t want to mess with that.
Once again, much of this is theoretical but needs immediate investigation.
Final Thoughts
Let’s see if I can wrap this all into a tighter package:
COVID-19 mRNA vaccines do not stay at the injection site, they circulate to many parts of the body including adrenal glands, liver, bone marrow, lymph nodes, ovaries, spleen, and thyroid and may stay there for up to 60 days. Spike protein may circulate in the body for up to 4 months.
Spike protein is toxic and suggested as a reason for certain COVID-19 symptoms and some of the reported vaccine adverse events.
The mRNA from the vaccines can be reverse transcribed into DNA (We are not certain this would happen in normal cells since the study was in vitro using cancerous liver cells).
IF the reverse transcribed DNA is taken up by the nucleus, whether it’s incorporated into the host cell or not, it COULD continue to express and cause ongoing production of spike protein and/or the gene sequences recently found (gp130 and MHS3).
IF all the above happens, it COULD cause a whole host of problems related to inflammation and DNA repair, including cancers, autoimmunity, reproductive issues, tissue inflammation (ex. myo/pericarditis), etc., etc., etc.
Some of these possible adverse events may not show symptoms for years after vaccination and therefore, never be linked back to the vaccines as causative.
One final time. Too be very clear, points 3-6 are almost entirely theoretical, but as I understand it, possible.
This all needs to be investigated ASAP!!
I would really appreciate reader feedback on this 2-part series from anyone well versed in such topics.
Have I understood the situation correctly? Are the concerns I outlined legitimate, in theory?