

Long-COVID-19 AKA Post-Acute Sequelae of SARS-CoV-2 (PASC)
Long-COVID-19 AKA Post-Acute Sequelae of SARS-CoV-2 (PASC)
It’s a real thing, but how prevalent is it and what is the cause?

I have recently been called anti-COVID (no surprise I guess) because of previous comments I made on Long-COVID (LC) in an earlier Substack article. Not that it bothers me all that much, this name calling is simply expected at this point. It did, however, get me interested to revisit the topic since my previous article barely touched on LC. So, I decided to write about it in more detail.
Before I even start, let’s make this very clear. LC is real. I never said it wasn’t, I simply made an argument, based on a peer-reviewed study, that it’s less of a concern than what the media and government would have us believe.
Many people don’t realize “long” symptoms can occur after nearly all transient viral infections we know about, Long-Influenza, Long-Cold, Long-etc. (1, 2) . You name the virus or bacteria and there is probably a long version of it documented in the medical literature. It even has a name. It’s called Post-Acute Sequelae (PAS). Therefore, in the scientific literature, LC is called Post-Acute Sequelae of SARS-CoV-2 (PASC).
The take-away point here is that PAS is not a new phenomenon that suddenly arrived with SARS-CoV-2, it has been known for a long time and there are multiple theories on why some people have “long” symptoms following the clearance of infections.
The main theory is that in some people the virus triggers chronic low-level inflammation in the body that remains after the virus is no longer detectable. Theories on why this happens to some and not others include: bacterial dysbiosis in the mucosa of the gut and/or respiratory tract, immune system exhaustion from ageing and other factors (ex. obesity, nutrient deficiencies, etc.), co-infections with other pathogens, autoimmune disorders triggered by initial infection, continual activation of the immune system by remaining, undetectable portions of the virus, or psychosomatic symptoms. These factors are likely not mutually exclusive and may all contribute to PAS in some way (1).
There are a large range of symptoms reported by PASC patients including: altered mental status, altered taste and smell, anxiety, ataxia, delirium, depression, dizziness, fatigue, headaches, memory loss,
nausea, new‐onset post‐traumatic stress disorder, seizures, strokes, tinnitus, sleep problems, joint pain, back pain, muscular pain, fatigue, poor attention or concentration, skin problems, sensory symptoms (pins and needles, tingling or burning sensation), hearing impairment, constipation, stomach pain, headache, breathing difficulties, palpitations, dizziness, chest pain, cough, and diarrhea (3, 4).
These are a wide range of symptoms that could be caused by a very wide range of things other than SARS-CoV-2, but since our society’s collective attention is almost entirely focused on COVID-19 people will automatically ascribe these symptoms to PASC without considering other possibilities.
Many older studies on PASC rely on symptom reporting from self diagnosed PASC patients with little to no focus on having proper control groups or the use of diagnostic testing. Below I will focus on 3 studies that address at least some of the shortfalls of some PASC studies.
Long-COVID Study #1
The first study I want to discuss attempted to compare neurological & psychiatric PASC with neurological and psychiatric symptoms of PAS-Influenza.
Out of the total population of test positive COVID-19 patients, only 2% reported PASC symptoms. Unfortunately, the study only includes flu patients that reported PAS so there is no baseline for determining what percent of flu patients end up with PAS-Influenza.
This study found that PASC and PAS-Influenza patients suffered similar symptoms, but the authors did not compare severity of symptoms based on participant reports. The only comment they make on this is that PASC patients were more likely to be prescribed pharmaceuticals for their symptoms, indicating that PASC may be more severe. Another explanation for this is that our society and medical system has such COVID-19 tunnel vision that physicians are more likely to prescribe for PASC than for PAS-Influenza, and PASC patients likely ask for drugs more often.
The most impactful part of the study for me was the results of laboratory tests between all groups. The authors are sure to mention multiple times that the lab results were significantly worse in the PASC vs PAS-Influenza groups, suggesting that PASC symptoms are more severe. However, the lab results from the COVID-19 positive, non-PASC group throws a wrench into that conclusion.
The lab results from those who had COVID-19 but did not develop PASC were worse than for those that did develop PASC. See the table below for your own reference.


So, if we take the results of all 3 groups into consideration, the lab values the study used are not actually reliable in determining symptom severity since the group with the worst results had no PAS symptoms.
These results should make us start to question the objectivity of PASC symptoms based on patient reports. Given the fear, panic, paranoia, and tunnel vision our governments and media have created around COVID-19, psychosocial factors should be a significantly important thing to investigate exhaustively regarding PASC.
**Before anyone bites my head off: This doesn’t mean subjective symptoms are not real or do not play a role in quality of life, but to learn how to effectively treat PASC we need to determine the real root cause(s).
On the psychosocial note, the study also found that the highest neuro/psych symptoms were depression and anxiety. While the study excluded anyone that had a previous history of diagnosed psychological health conditions, we know there are many people who have such conditions, or prone to them, without being formally diagnosed. So, was it the people with undiagnosed psychological conditions or those that are more prone to them that more often suffer from PASC? It’s a great question but it was not addressed in the study.
Additionally, PASC was associated significantly more with females even though women are less likely to have severe COVID-19. There is a good deal of evidence that women are nearly twice as likely to suffer from anxiety (this is not sexist and easy to search online on your own). This lends more evidence to the involvement of psychosocial factors, and PASC possibly being, at least partially, psychosomatic. Keep this in mind while we have a look at the next 2 studies.
**Before anyone bites my head off again: This doesn’t mean psychosocial factors are the only thing at play it just needs to be strongly considered and investigated.
Long-COVID Study #2
A study that was originally published in early November 2021, found that the belief in having COVID-19, was a better indicator of physical PASC symptoms than actually having test confirmation of COVID-19.
This study included a cohort of 26,823 participants and focused on physical symptoms only. The presence of physical PASC symptoms was present in 0.6-10.4% of participants, depending on the symptom.
The study asked participants if they previously had COVID-19 (yes/no), if they had a laboratory test confirming COVID-19 infection (yes/no/type) and whether they experienced any of 18 possible symptoms associated with PASC. The authors also confirmed previous COVID-19 infection through serological testing (antibodies).
The results showed that the belief in having COVID-19 (based on serological testing) was associated with higher odds of having all 18 physical PASC symptoms while confirmed COVID-19 infection was only associated with anosmia (partial or complete loss of smell). When the authors adjusted for self-reported health status and previous symptoms of depression, the results remained consistent.
Since this study also included participants who did not have confirmed or reported COVID-19 but still completed the PASC physical symptoms questionnaire, it was one of the first studies to include a control group. The results showed that all 18 physical PASC symptoms occur frequently in the general population (no relation to COVID-19 infection). Therefore, the authors suggest that physical PASC symptoms may not be caused by SARS-CoV-2 infection.
Here are some concluding remarks from the study:


As I mentioned above, to properly treat the attributed symptoms of PASC, it shouldn’t be automatically assumed they are caused by COVID-19 and proper diagnostic testing and medical examination should be done. Take off the COVID-19 blinders and find the root cause for each individual patient.
**Before anyone bites my head off for a 3rd time: Yes, these symptoms could be PASC for some people, but it’s almost certainly not the case for everyone claiming PASC. Doctors are doing their patients no favour by assuming PASC. Find the root cause for each unique individual and treat appropriately. Take of the blinders. I am sure some physicians are doing this, but I’m not sure the public is getting the message.
Long-COVID Study #3
A study published in May of 2022 of 189 participants with laboratory confirmed previous COVID-19 and 122 control group participants with no history of COVID-19 (similar in demographic characteristics) found only 2 risk factors associated with increased odds of reporting PASC. These risk factors were a self-reported history of an anxiety disorder and being female. Seems to be in line with what the above 2 studies implied.
The great thing about this study is that they also used physical examination and multiple, objective, diagnostic tests. Blood work included routine chemical analysis; hematologic assessment; measurement of D-dimer, high sensitivity C-reactive protein, rheumatoid factor, antinuclear antibody, anticardiolipin antibodies, troponin I, pro–B-type natriuretic peptide, serum immunoglobulins, and SARS-CoV-2 antibodies; and research evaluations of immunologic parameters. Additionally, participants underwent neurocognitive assessments, pulmonary function testing, a 6-minute walk test, and an echocardiography.
While 55% of the COVID-19 cohort reported at least 1 PASC symptom and only 5% of the non-COVID-19 cohort reported at least 1 of these symptoms, none of the objective diagnostic testing listed above was significantly different between the 2 groups.
This means that extensive, objective diagnostic testing did not reveal an objective cause for PASC symptoms. In combination with previous anxiety disorders and female sex being the only risk factors for PASC, these are interesting findings. The authors conclude their paper as follows:

**Before you bite my head off for the 4th time: Yes, subjective symptoms can have an impact on quality of life but treating all PASC patients by assuming their symptoms are caused by previous COVID-19 infection (without objective testing) is not doing them any favours.
Conclusion
Between 2% and 55% of people report experiencing PASC symptoms following COVID-19 recovery. These are important findings in and of themselves as they relate to quality of life. However, the root causes of these symptoms may not actually be SARS-CoV-2 infection based on the above studies. These are also important findings because to effectively treat PASC patients, there needs to be a solid understanding of the root cause.
I agree that for some people PASC may in fact be due to SARS-CoV-2 infection, but this cannot be assumed. Diagnostic testing should be performed so these individuals can be treated properly.
The studies discussed above suggest that anxiety disorders, or those who may be prone to such disorders, may be the key to predicting PASC, and for many patients exhaustive diagnostic testing is negative for any objective cause of PASC. These results suggest that many PASC patients are experiencing psychosomatic symptoms, which is defined as physical symptoms manifesting from psychological factors.
So, of the 2-55% of COVID-19 patients that report PASC, what percentage of them are likely to be experiencing something closer to psychosomatic symptoms?
The results from the last study discussed above reveal that 48% of the PASC group had a previous mental health condition.
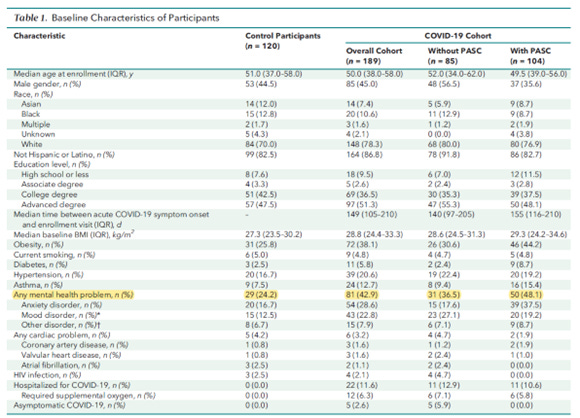
On its own, this doesn’t prove that 50% of PASC patients have a psychosomatic disorder and are being treated inappropriately, but it certainly lends evidence to that theory. Additionally, the study found that 44% of PASC patients were obese, which can cause many PASC symptoms independently of SARS-CoV-2 infection.
The above 3 studies suggest that many factors are at play in PASC, many of them having nothing to do with SARS-CoV-2 infection since PASC symptoms are very common in the public and caused by conditions that also increase the risk of getting COVID-19 (ex. obesity). In addition, close to 50% of PASC cases could possibly be attributed to psychosomatic symptom.
All thing considered from these studies, I think it could be argued that at least 50% of PASC patients have symptoms that have nothing to do with actual SAR-CoV-2 infection and are thus not likely being treated properly.
The Following is Just My Current, Humble, Non-Expert Opinion.
Our government and media have whipped much of the population into a panic with constant fear messaging about COVID-19. North America was already experiencing a mental health crisis and the pandemic policies (lockdowns, quarantine, isolation, etc.) have been proven to exacerbate this problem.
Now we have a large portion of the population with previous anxiety disorders, those with newly diagnosed anxiety disorders because of pandemic policies, and many who have been pushed closer and closer toward such disorders because of pandemic policies.
Next, the government and media tell us that it’s not just the acute COVID-19 symptoms you need to worry about, there is also a significant risk of LC symptoms. On top of that, these symptoms match a whole host of symptoms from a wide range of other medical conditions that were common well before the pandemic.
This seems like the perfect storm for psychosocial factors being a major cause of PASC, and I blame the government and media for this. And the medical professionals who know better and don’t speak up. I believe a lot of pain could have been prevented on this front.
PASC seems like a good excuse for all that ails us, meaning we don’t have to blame ourselves for any health problems we may have. It’s a nice easy way out of taking the necessary steps to get healthier.
Is it possible the government and media have actually conjured PASC into existence with their messaging? I am not the only one who thinks so.

What do you think?
Don’t’ forget
To be clear, I think PASC is very real for some. However, it’s frequency appears to be exaggerated since many PASC sufferers experience symptoms for reasons other than SARS-CoV-2 infection, such reasons are not properly investigated, and therefore people may not be receiving proper treatment.